The Silent Scream of the Median Nerve: Navigating the Carpal Tunnel Maze
It starts as a whisper. A vague numbness in the thumb after a long day typing; a strange, prickling electric vibe buzzing through your index finger at 3 AM that shakes you awake. You shake your hand out, the feeling returns, and you ignore it.
But the whisper becomes a shout. Soon, it’s not just annoying; it’s clumsy. You drop your coffee mug. Buttoning a shirt feels like doing microsurgery with oven mitts. This isn't just fatigue. This is Carpal Tunnel Syndrome (CTS), a physiological traffic jam in the most critical junction of your hand.
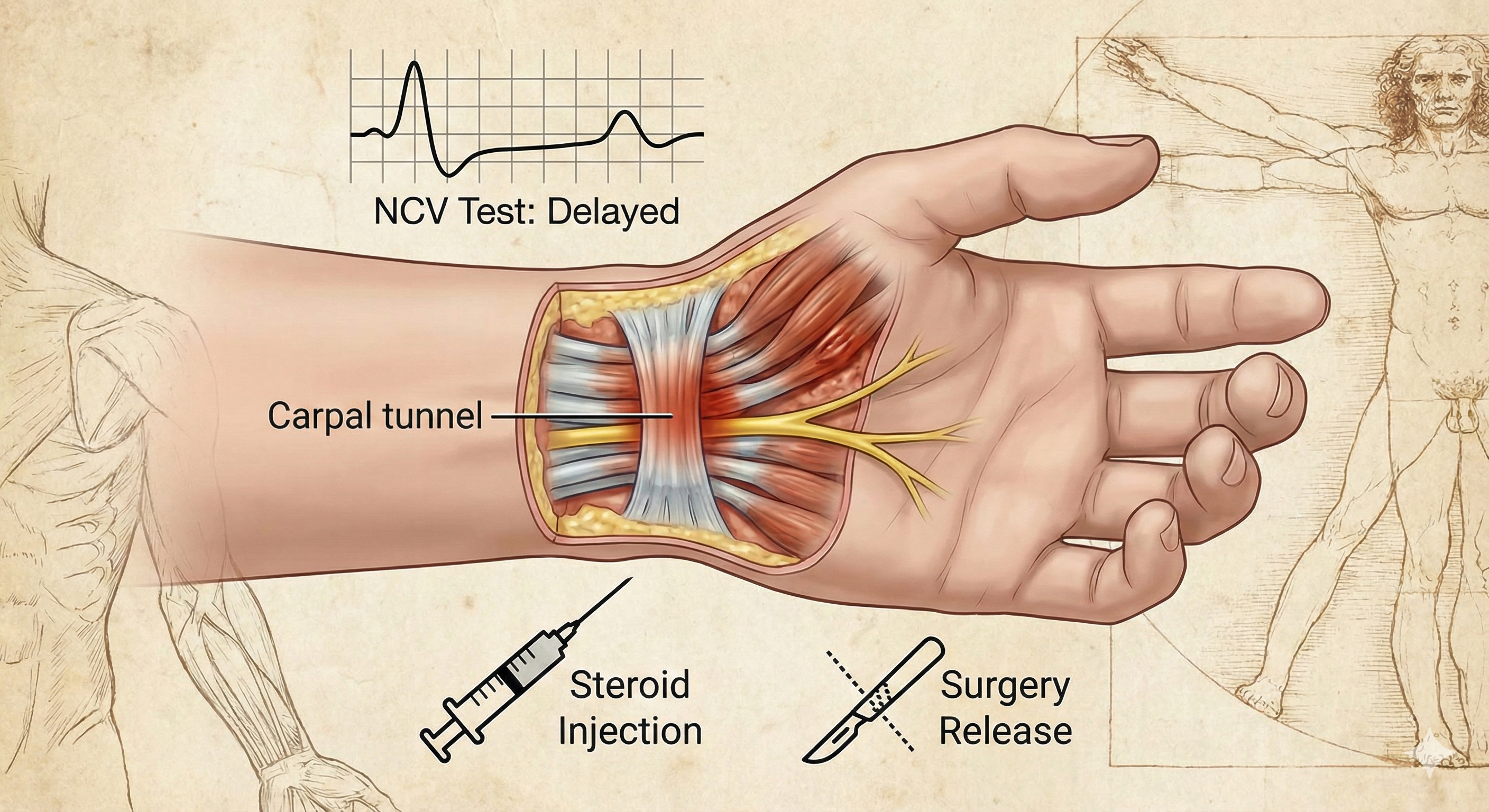
CTS is fundamentally a space issue. Your wrist contains a narrow passageway the carpal tunnel housed by rigid bones and a tough ligament roof. Crowded inside are nine tendons and the star of the show: the median nerve. This nerve is the information superhighway controlling sensation and muscle movement for much of your hand. When inflammation from overuse, anatomy, or underlying conditions swells those tendons, the tunnel doesn't expand. The median nerve gets choked.
The result? Pain, weakness, and a slowly disconnecting limb.
The Electrician’s Truth: Why You Need the NCV Test
You tell your doctor your hand is numb. They tap your wrist (Tinel’s sign) and bend it backward (Phalen’s maneuver). Tingles erupt. It looks like CTS. It smells like CTS. But is it definitely CTS?
Clinical tests are mere indicators; they can be fooled by pinched nerves in your neck or diabetic neuropathy. You cannot fix what you haven't definitively identified.
Enter the Nerve Conduction Velocity (NCV) test, often paired with an EMG (electromyogram). It is the gold standard. It is the difference between guessing and knowing.
Think of your arm as a house and the nerves as the electrical wiring. The NCV test is the master electrician showing up with a voltmeter. By placing surface electrodes on your skin and delivering small, brief electrical shocks, the test measures exactly how fast or painfully slow electrical signals are traveling down that median nerve highway.
If the signal hits the wrist and suddenly hits bumper-to-bumper traffic, slowing down significantly compared to other nerves, the NCV provides irrefutable, quantitative proof of the compression. It tells us not just if you have CTS, but how bad the wreckage is.
Managing the Squeeze: From Splints to Steroids
The management of CTS is a ladder of escalation. You don't jump to the top rung unless the building is already on fire.
Early Stages (Mild CTS): The symptoms come and go. The NCV shows only minor slowing. Here, we play defense. Nocturnal wrist splinting is paramount—it stops you from bending your wrist in your sleep, crimping the nerve like a garden hose all night. Ergonomic adjustments and anti-inflammatory pills (NSAIDs) are the standard foot soldiers in this early battle.
The Middle Ground: The Role of Steroidal Injections This is where the magic and the controversy often lies.
If splinting fails and the NCV shows moderate conduction delay, but your muscles still work fine, corticosteroids enter the chat. These injections are powerful, targeted anti-inflammatory bombs dropped directly into the carpal tunnel.
When are they given? Usually in the mild-to-moderate stages where pain and acute inflammation are the dominant features. They are excellent diagnostic tools as well; if an injection stops the pain cold, it confirms the diagnosis.
What do they do? They shrink the swollen tissues surrounding the nerve, buying the median nerve precious breathing room.
The Caveat: They are often temporary. For some, relief lasts years; for others, weeks. They put out the fire, but they don't widen the fireplace. Doctors usually limit these to a few per wrist, as overuse can weaken tendons.
The Final Frontier: When Surgery is Inevitable
Nobody wants surgery. But sometimes, it is the only path to salvation for the nerve.
If you ignore CTS, the median nerve doesn't just get irritated; it begins to die. The NCV test will show severe blockage or even signal absence. You might notice the meaty part of your thumb (the thenar eminence) starting to shrink and flatten. Grip strength vanishes. The numbness becomes constant, not intermittent.
This is the severe stage. Steroids are useless here; the damage isn't just inflammation anymore, it's structural compression.
At this critical juncture, Carpal Tunnel Release surgery is required. It is a structural fix for a structural problem. The surgeon cuts the transverse carpal ligament the roof of the tunnel. Instantaneously, the pressure is gone. The tunnel springs open, and the median nerve can finally breathe.
While recovery takes time, for severe cases, it is the only way to prevent permanent nerve damage and claw-hand deformity. Listen to the whispers in your wrist before they become screams that require a scalpel to silence.
Still have questions about your symptoms?
Get a professional diagnosis from Dr. Bhupesh Kumar. Early detection leads to better recovery.
Book ConsultationShare this article: