Headache: When to Worry and When to Breathe
It Is Not Always Just Stress
Everyone has had one. That dull, grinding pressure behind the eyes at the end of a long day. The throbbing that starts at the temples and spreads like a slow tide. The headache that arrives quietly and refuses to leave. Most people reach for a painkiller and move on. That works. Until it does not.
Here is the uncomfortable truth: a headache is both the most common neurological symptom in the world and the most frequently under-investigated. Patients dismiss it. Doctors sometimes do too. And in that dismissal, real diagnoses get missed.
This is not a post designed to alarm you. It is designed to make you smarter about something your brain does, because yes, sometimes your brain is literally the source of the pain, and sometimes it is desperately trying to signal you.
Let us talk about it properly.
The Anatomy of Pain You Cannot See
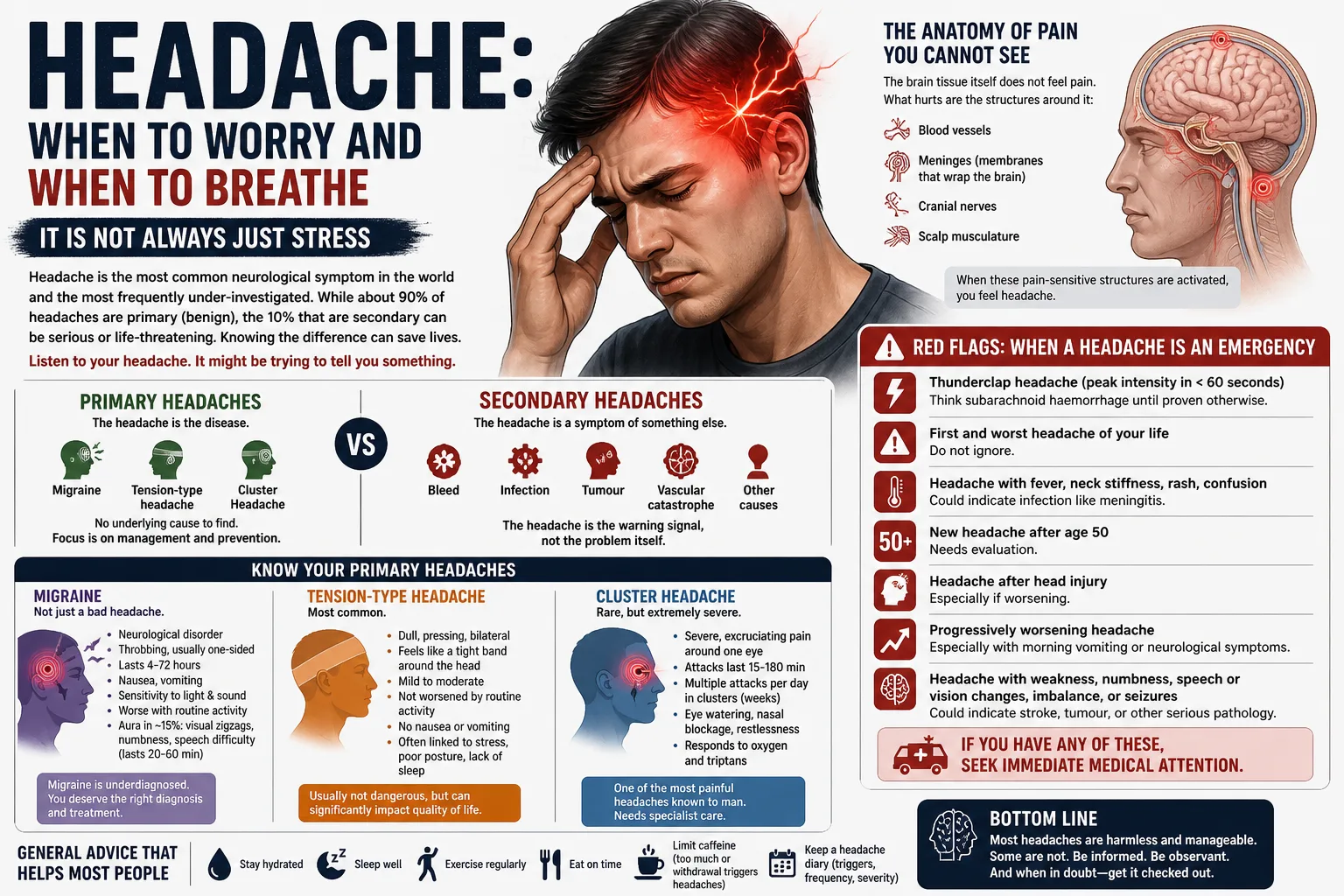
Your brain itself does not feel pain. That is not a typo. The brain parenchyma (the actual brain tissue) has no pain receptors. What does hurt are the structures around it: blood vessels, meninges (the membranes that wrap the brain), cranial nerves, and the scalp musculature.
So when you have a headache, something is activating those pain-sensitive structures. The question is what.
This is why headache medicine is not simple. It is not one condition. It is a universe of conditions that all produce the same symptom: head pain. The diagnostic job is to figure out which universe you are in.
Primary vs Secondary: The Most Important Divide
Every headache in medicine falls into one of two broad categories.
Primary headaches are conditions in themselves. The headache is the disease. Migraine. Tension-type headache. Cluster headache. There is no underlying cause to find because the headache disorder is the diagnosis.
Secondary headaches are symptoms of something else. A bleed. An infection. A tumour. A vascular catastrophe. The headache is the warning signal, not the problem itself.
Here is the brutal truth: about 90% of all headaches are primary. They are benign in the sense that they will not kill you. But the 10% that are secondary? Some of those are emergencies. Some are life-threatening within hours.
The clinical art is sorting which is which. And it starts with listening to the headache's story.
Migraine Is Not Just a Bad Headache
Let us spend time here because migraine is the most misunderstood condition in neurology.
Migraine is not "a really bad headache." It is a neurological disorder. A brain state. During a migraine attack, there is a wave of electrical activity followed by suppression that spreads across the cortex, a process called cortical spreading depression. Neurotransmitter systems, particularly involving serotonin and calcitonin gene-related peptide (CGRP), are dysregulated. The trigeminovascular system is activated, which is why the pain is typically throbbing, typically one-sided, and often accompanied by nausea, vomiting, and sensitivity to light and sound.
Migraine makes you want to lie in a dark, silent room and wait it out. That is not weakness. That is neurobiology.
About 15% of migraineurs experience aura, a set of reversible neurological symptoms that precede the headache: visual zigzag lines (fortification spectra), numbness spreading across one side of the face or hand, or rarely, a brief difficulty with speech. Aura lasts 20-60 minutes and resolves. It can be terrifying the first time it happens, often mistaken for a stroke or a TIA.
Migraine is also significantly underdiagnosed in India. Many patients with migraine have been told for years that they have a "sinus problem" or "weakness headaches." They have been on antibiotic courses for rhinitis that was never present. They have taken decongestants that made no difference because the sinuses were never the issue.
If your headache comes in attacks, lasts 4-72 hours, is pulsating in quality, is worsened by routine physical activity, and is accompanied by nausea or light/sound sensitivity, you likely have a migraine. You deserve a proper diagnosis and a proper treatment plan.
Cluster Headache: The Headache That Breaks People
Cluster headache is rare. But if you have it, you know it.
The pain is described by patients as a red-hot poker being driven through one eye. It comes in clusters: multiple attacks per day, for weeks at a time, then disappears entirely for months. Each attack lasts 15-180 minutes. During an attack, the eye on the affected side waters. The nostril runs. The eyelid droops. The patient is typically agitated, unable to sit still, pacing, sometimes hitting their head against a wall to distract from the pain.
This is not exaggeration. This is the reported patient experience. Cluster headache has, in chronic sufferers, one of the highest rates of suicidal ideation of any pain disorder.
It responds poorly to standard pain medications. High-flow oxygen (100% at 12-15 L/min via non-rebreather mask) can abort an attack. Subcutaneous triptans work. Prevention during the cluster period requires specialist input.
If anyone around you describes this pattern, do not send them home with a paracetamol prescription. Send them to a neurologist.
The Red Flags: When a Headache Is an Emergency
Medicine has a saying: the worst headache of your life may be the most important one you ever report.
Thunderclap headache (onset to maximum intensity in under 60 seconds) should be considered a subarachnoid haemorrhage until proven otherwise. This is a bleed from a ruptured aneurysm in the subarachnoid space. It carries a high mortality. It presents as sudden, explosive, severe head pain, sometimes described as a "blow to the back of the head." Urgent CT and lumbar puncture are required.
Other red flags that mandate immediate investigation:
- Headache that is the "first and worst" of a patient's life
- Headache with fever, neck stiffness, and photophobia (think meningitis)
- Headache with focal neurological deficit: one-sided weakness, slurred speech, vision loss
- Headache in a patient over 50 with no prior headache history, especially with scalp tenderness or jaw pain (temporal arteritis must be excluded)
- Headache worsening progressively over weeks, worse in the morning, worse with bending forward or coughing (raised intracranial pressure)
- Headache after head trauma
- Headache in a patient with known cancer or HIV
None of these are panic triggers. They are clinical prompts. They mean: do not treat empirically and wait. Investigate first.
What a Neurologist Actually Does for Headache
When you visit a neurologist for headache, the process is more detailed than a GP appointment and for good reason.
The consultation involves a structured headache history: age of onset, frequency, duration, character of pain, location, associated symptoms, triggers, relieving factors, family history, and medication use. The last point matters because medication overuse headache is a real and underappreciated condition, where taking acute pain relief (even paracetamol) on more than 10-15 days per month transforms episodic headache into daily chronic headache.
A clinical neurological examination is performed to rule out secondary causes.
Investigations may include MRI brain (with and without contrast), MRA (MR angiography of the cerebral vessels), EEG if seizures are a concern, or blood tests including inflammatory markers if vasculitis is suspected.
For migraine, treatment involves two tracks: acute (aborting an ongoing attack) and preventive (reducing frequency and severity over time). Preventive options include beta-blockers, topiramate, amitriptyline, CGRP antagonists, and in refractory cases, procedures such as sphenopalatine ganglion (SPG) modulation or botulinum toxin injections.
Headache management is not one-size-fits-all. It is personalized neurology.
The Takeaway
Headache is common. It is also complex. It ranges from the benign but debilitating (migraine, cluster) to the immediately life-threatening (subarachnoid hemorrhage, meningitis).
Do not normalize a headache that is changing. Do not accept "it is just stress" if your pain is frequent, severe, or associated with any neurological symptom. Do not self-medicate for months without a diagnosis.
Your brain is worth investigating.
Still have questions about your symptoms?
Get a professional diagnosis from Dr. Bhupesh Kumar. Early detection leads to better recovery.
Book ConsultationShare this article: